Fact check: does Astra Zeneca's COVID-19 vaccine increase risk of thromboembolism
Before I begin, I probably need to declare that although I'm a great enthusiast of vaccinations and got a more or less complete list of shots in my life, none of the pharma companies nor Bill Gates have ever offered me shares, honoraria or even a free vaccination. In other words I'm entering this topic highly influenced by subjective opinions and conspiracy theories without any financial conflict of interest and do my best to present you 100% scientific data.
COVID-19 vaccination was promised to be the next topic - it was already a while ago, cause I'm involved in two huge COVID-19 human studies and didn't find enough time for my blog. But I hope, I can report on our, still highly confidential, results in the nearest future.
Initially I thought: let's discuss the principle of vaccination and particular drugs, have a look what was published about efficacy and safety and, finally calculate, if getting an anti-SARS-Cov2 shot is worthwhile. But, I didn't expect to begin the series with a topic handling severe adverse events. Somehow I'm obliged to do so, cause I recommended the 'poor-man' Astra Zeneca vaccine to few people and I hope I can soothe your doubts and concerns.
Fast primer: Astra Zeneca is a vector vaccine
Astra Zeneca's vaccine, known also as AZD1222 or under its commercial names Vaxzevria and Covishield, is a viable adenovirus-based shot, so called vector vaccine. Adenoviruses, like those inside the drug, are extremely common pathogens causing upper respiratory, cold-like infections. You don't have to worry: you had already plenty of them during your childhood and against many your body has robust neutralizing antibodies. There's another reason, why AZD1222 is not going to kill you: the virus inside can efficiently infect multiple cells of your body but due to removal of few viral genes it can't copy itself: you're likely to feel quite sick for a day or two, but that's all.
Well, but, what the adeno has to do with corona? Adenoviruses possess a DNA genome, which they place into the nucleus of an infected cell and let the cell produce viral proteins. In case of the vaccine virus, the genome codes the spike protein of SARS-Cov2 and the infected cell is going to manufacture it and show on it's surface. Such 'fake-spike' is supposed to induce potent immune response - not only antibodies but also so called killer/cytotoxic T cells, which will finally eliminate the adeno-infected cell, and in the future any cell hosting the pathogenic SARS-Cov2. So if you had heard that the pharma lobby and Gates' Foundation is planning to genetically modify humans with vaccines - yes it's somehow true for this vaccine: you or, more precisely, few of your cells will be genetically modified by the adeno-vector for some time. But remember: any virus which you get from your friend of kindergarten kid will do exactly the same! And your immunity will finally cope with this problem.
The Astra Zeneca vaccine has many apparent problems...
You may find the mechanism of action sketched above quite elegant. And vector vaccines, there are more of them coming: Sputnik V and Jonhson & Johnson belong to the same group, have also much more advantages: they are cheap to produce, the adeno-genome is easy to modify (believe me: I used to work with it as a young scientist!), easy to store and transport. However, they have few weaknesses as well:
- Adenos are immunogenic, i.e. they induce antibodies not only against the spike protein of the corona but also against themselves. Once you have them, the boosting vaccination is likely not to work as good as the first shot. Your immunity will destroy the vaccine vector instantly upon entry into your body
- Vector vaccines seem not to be as effective as RNA vaccines at preventing SARS-Cov2
- There's at least one vaccine-resistant SARS-Cov2 variant, B.1.135.
- The magnitude of immediate side effects is stronger that for e.g. 'rich-men' RNA vaccines
- There are huge delivery delays which endanger the pan-european vaccination program
As usual, I'm going to investigate the root of this controversy in light of the published data. As you will see in a moment, from a statistical point of view, there's no doubt that the drug is safe. And as you will see, it's not so obvious from the political and ethical point of view.
The analysis scripts are available here. In my analyses I'll focus on data published for Germany, since the issue seems to be most weighty there. My data sources concerning the number of vaccinations, sex and age distribution and frequency of thromboembolism: press releases, safety reports issued by the Germany's vaccination authority, Paul-Ehrlich Institure. One issue with those data refers to the number of vaccinations with Astra which is correct as of 12th March, the number of the severe adverse effect cases refers to the press release on 30th March; the risk of thromboembolism is hence a bit overestimated (up to factor 2), which however has no impact on data interpretation. The studied populations are narrowed down to the age interval of 20 to 59 years as all the cases in Germany were found there (population counts from 31.12.2018 from www.bpb.de). COVID-19 incidence and mortality data as of 23th March were obtained from statista.com and the dashboard of the Robert-Koch Institute. Yearly prevalence of venous thrombosis in Germany for the population aged 18 to 65 was extracted from the paper by Ohlmeier and colleagues - in this case I considered the worst case scenario provided.
Is thromboembolism one of them?
I have to admit, I had to think a while how to crunch this data. First of all, there's not much known on the prevalence of similar thrombotic events in the general population. Second, when talking on the trade-off between safety and efficacy of a vaccine, we need to compare apples and pears (thrombosis cases versus COVID-19 deaths), which is not what a statistician likes most. Nevertheless, I'll try my best.
Till yesterday (30th of March) for the period from 27th January on, German press reported on a total of 31 severe cases of thromboembolism in people vaccinated with AZD1222: 29 in women and 2 in men, all of them less than 60, and nine of them died. All the cases happened between day 4 and day 16 post immunization. Importantly, till 12th of March, roughly 860 000 women and 405 000 men in this age class got at least one shot of the drug. Of note, in Germany, the AZD1222 vaccine was administered mostly to production-age female front-line workers: health care professional and teachers, which explains the huge disproportion between sexes.
As you may appreciate in Figure 1, the risk of such nasty adverse event is extremely low: and lays far below one tenth of promille - approximately 3 to 4 women out of 100 000 and 1 men out of 100 000 will experience it. Please
consider: by looking at the mere size of the vaccinated German
population you have to admit this is an extremely rare adverse effect and there was no chance to record it in the approval relevant clinical studies with the drug which included less that 25 000 participants! But how does it relate to other case thrombotic events? or COVID-19 deaths assumed that the entire vaccinated group gets COVID-19? This is not so obvious as it seems and depends critically on the observation time we set for such comparison. If we assume that the vaccine-related thromboses occur within 2 weeks post vaccinations, we need to fetch 14 day COVID-19 mortality and 14 day incidence of venous thrombosis as comparators (Figure 1A). However, if we agree that the vaccination program with AZD1222 has been running for roughly 3 months now, we need to compare the thrombosis rate to 3 month (quartal) mortality and thrombosis incidence (Figure 1B). In any case, the incidence of thrombotic events upon vaccination stays far below the expected risk of any-case thrombosis in Germany! But, the only figure of vaccine-independent thrombosis incidence provided by Ohlmeier et al. refers to a broad spectrum of thrombotic events, most of which don't require hospitalization or does not pose a risk of death. Because of that, the risk of the adverse event in the vaccinated women within the 14 day observation period may easily exceed the expected number of the life-threatening thrombosis in the general population below 60. This was pointed out also in the recent release by EMA. For men, I don't expect such a phenomenon.

Figure 1. Risk of experiencing a thrombotic event after the AZD1222 vaccine, any-case venous thrombosis and death after COVID-19 infection in women and men aged 20 to 60 years in Germany. (A) Within the 14 day observation period. (B) Within the 3 month observation period. Reference population sizes: vaccinated women n = 860 000, vaccinated men n = 405 000, women in Germany n = 21 700 000, men in Germany n = 22 600 000, COVID-19 infected women within 14 days n = 34 200, COVID-19 infected men n = 32 200.
What about the COVID-19 mortality? It's in turn substantially higher for men than women and oscillates between 1 and 2 promilles. This means, if the whole vaccinated collective were infected with SARS-Cov2, we could expect almost 800 deaths among females and roughly 1800 male fatalities during the whole pandemic. So, trading the severe adverse effects against the mortality in the whole one year pandemic setting strongly suggests that vaccinated is less risky per se than getting COVID-19 - and you see it clearly in Figure 1.
Till now our conclusions seem to follow sound logic - which is not enough if we want to know what's the chance that those 31 thrombosis cases are simply a coincidence, bad luck or an anomaly. In order to estimate that, we need a robust modeling approach. If you are a data professional, you'll immediately point out several of them: bootstrap, binomial test or, in my case, Poisson test. I found the nicest explanation how such test works at Cross Validated. In brief, it compares the event frequency in the test sample, in our case the vaccinated collective, with the event frequency in the reference population, for us the general German population and COVID-19 infected subjects. Applying this method, I can obtain the estimated frequency in the sample assuming it behaves like the reference population - and get the data presented in Figure 2.

Figure 2. Results of Poisson modeling: expected cases of thrombosis and COVID-19 deaths in the vaccinated population if it gets infected (orange) versus the number of severe thrombotic events after vaccination (beige). (A) Within the 14 day observation period and (B) within the 3 month observation period.
For the 14 day observation interval (Figure 2A), I expect to see 66 cases of women with thrombosis independently of the vaccination and 456 cases if I extend the window to 3 months (Figure 2B) - the incidence in the vaccinated group is clearly below the population mean!!! As discussed above, it may change, if we focus on the particular type of thrombotic events observed after the immunization. But again, rather not for men. A quite similar conclusion can be drawn for the COVID-19 fatality. Importantly, due to the test result, the departure from the population means is also extremely significant for both observation time: low p values and confidence intervals represented by whiskers far below one (Figure 3) speak for safety of the vaccine and an excellent benefit-to-cost ratio.
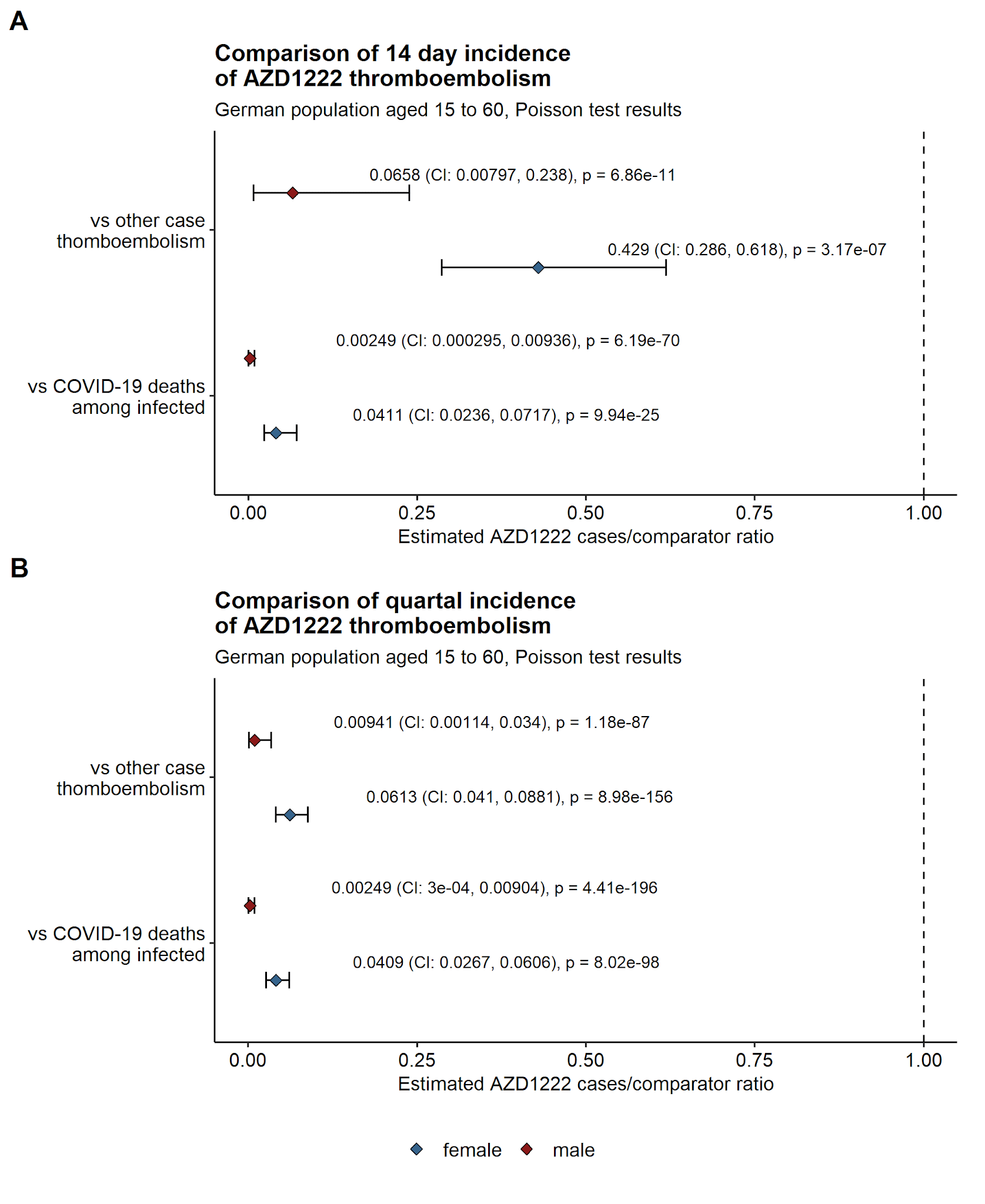
Figure 3. Results of Poisson modeling: estimated ratio of events (any-case thrombosis and COVID-19 deaths) in the vaccinated sample to the observed event count in the reference population.
(A) Within the 14 day observation period and (B) within the 3 month observation period. Diamonds represent estimated ratios, whiskers stand for 95% confidence intervals. P values indicate the probability that the observed departure from sample:population ratio of 1 is happens at random. Note: diamonds below 1 show lower event frequency in the vaccinated sample than in the reference population.
In sum: the data we have now suggest with huge confidence that the AZD1222 Astra Zeneca's vaccine is safe for women and extremely safe for men from a statistical point of view. The frequency of thrombosis is likely below the any-case thrombosis found in the general population and the expected number of COVID-19 deaths prevented by the drug clearly outweighs the risk of severe thrombosis. So if you ask me if I let myself vaccinated one day (most likely next year, looking at the pace of EU's vaccination campaign) with Astra Zeneca: yes, 100% sure.
Even a rare adverse effect matters when it comes to a mass-use drug
Having said that I also fully understand one's concern or refusal to get vaccinated with the Astra Zeneca's shot. Fortunately we are lucky enough to live in a comfortable western world and, apart from corona nowadays, none of us is used to weight the life or health risk against benefit. You don't have to consider if a glass of tap water may kill you with a probability of 1:100 000 or a piece of Tyrolean cheese may harbor few nasty bacteria which will send you to hospital with a probability of 1:50 000. Paranoid, isn't it? We are accustomed to the extreme safety of our water, food and common use drugs such as pain killers, hypertension drugs or contraception and we trust the authorities which control and approve them. Of course there are few sad examples of mass-use things harming our health and shortening life: alcohol, tobacco, diesel engine, but since they kill us slowly, we learned to ignore them.
Anti SARS-Cov2 vaccines are thought to be such mass-use drugs. We're planning to immunize all adults, reach in a record-breaking time the herd immunity and refresh the vaccination as soon as the antibody level drops or an immune-escape virus emerges. This utopia requires billions of vaccines being produced and administered each year. As a single individual you'll get one at the onset of the annual COVID-19 season up to 60 - 80 times in your life. Such a vaccine needs to be absolutely safe to an insane degree!!! Otherwise you have a political problem - less in a small country like Austria where one to five severe side effect cases per year won't probably fuel a medial outreach and more in Germany or US where the cases may exceed hundred. In addition: vaccinations are an ideal butt of pseudo-science and conspiracy theories. Approving a shot which is not absolutely safe will let the conspiracy scene grow even further and undermine the credit of state's authorities suffering anyway in this crazy pandemic time...
Back to the vaccination risk and size of German female population between 20 and 60 (Figure 1) - there are over 20 million people to vaccinated primarily with the AZD1222 drug. As clearly stated by PEI and STIKO (Ständige Impfkommison), there's a likely causal link between the vaccination and extremely rare atypical blood clotting events. So, considering the extra risk of severe thrombosis in 1 to 4 women per 100 000 after the AZD1222 vaccination, one may expect somehow between 200 and 800 cases needing hospitalization and at life risk alone after the first dose. Politically it's not acceptable and I also fully understand the STIKO's recent decision not to recommend the shot for people below 55. At the same time I have to stress that the drug seems to be really extremely safe and effective in elderly with an even larger benefit in terms of prevented COVID-19 deaths. This new recommendation will hence likely accelerate the hitherto snail-slow EU's vaccination campaign in the most prominent vulnerable group.
What does it mean for you?
Even though I trust my data and attest the Astra's product safety and efficacy, this is a hot topic at home: many of colleagues and friends in the health care sector got already the first AZD1222 shot, for many middle age people, including the blog author, the Astra's vaccine is the most probable one to get in the future. There are few common sense recommendations you can follow and talk to a physician if one of the issues below refers to you:
- you are female under 60
- you take oral contraception or hormone-replacement therapy
- experienced blood coagulation problems in the past
- you smoke, have obesity, diabetes, atherosclerosis or hypertension - these conditions are often associated with pathological blood clotting
- you had COVID-19 in the last 6 months
If you already got a shot: once you feel sick for 4 days or longer straight after the vaccination or get fever, abdominal or chest pain, blue patches on the skin, blue fingers or toes or a reticulated (net) rash, acute headache, vision or neurological problems a while after the shot: don't wait and call the emergency! If recognized rapidly, your thrombotic event is perfectly curable!
Stay healthy!
Comments
Post a Comment